
Melanotan is a peptide being studied for its various research applications, including skin tanning and sexual health.
Melanotan is a synthetic analogue of alpha-melanocyte-stimulating hormone, or α-MSH for short. α-MSH is one of a number of melanocortin peptide hormones in the body [1]. Melanotan is typically injected or administered as an implant and binds to melanocortin receptors 1, 3, 4, and 5.
There are two types of melanotan molecules: melanotan I and melanotan II. They have both been linked to increased melanin production and increased tanning of the skin [2, 3, 4, 5, 6, 7].
While there is strong research interest in both melanotan molecules, this review will focus on melanotan I.

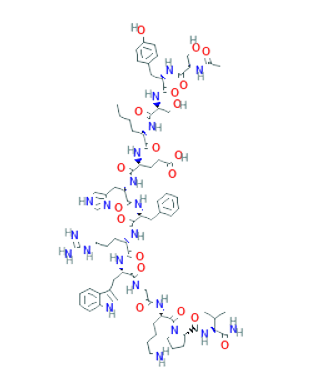
Melanotan I ([Nle-D-Phe]-α-MSH) is a synthetic peptide that has a linear formation. It is 13 amino acids in length and has the same structure as α-MSH save for two key differences. First, the fourth amino acid in melanotan I is norleucine; second, the seventh amino acid is D-phenylalanine [5].
In the body, melanotan I primarily binds with the MC1R receptor and is more potent and resistant to breakdown than α-MSH [7]. Studies have shown that MT-1 significantly enhances tanning and reduces sunburn [4].
Melanotan I should not be confused with melanotan II (Ac-Nle-[Asp-His-D-Phe-Arg-Trp-Lys]- α-MSH-NH2). MT-2 is less receptor-specific than melanotan I and has been linked to more side effects. Studies have shown that melanotan II increases libido and decreases appetite to a greater extent than MT-1 [6].
A number of clinical trials have evaluated the safety and efficacy of melanotan I, from which the following benefits can be drawn.
Melanotan I binds to the melanocortin 1 receptor (MC1R), thereby increasing melanin production. This has the secondary effect of increasing levels of the enzyme tyrosinase and melanocyte [2, 3]. Studies have found that MT-1 can increase the rate of tanning and reduce the number of sunburnt cells in test subjects [4].
Three phase I clinical trials conducted by dermatology clinics at the Arizona Health Sciences Center have investigated two dose levels of melanotan I combined with small doses of UV-B to the neck or buttock, or full sunlight to half of the back. In these trials, test subjects receiving melanotan I had 47% fewer sunburn cells on their neck and “significantly enhanced tanning” on their back compared with the control group [4].
Results from several phase II clinical trials sponsored by Clinuvel Pharmaceuticals have shown that melanotan I offers psychological benefits including improved mood and outlook in patients who had received photodynamic therapy (PDT), a treatment that uses light and photosensitization to kill cancer cells [5].
A 2008 phase II multicentre, double-blind, placebo controlled pilot study aimed to evaluate whether melanotan I implants (referred to in the study as afamelanotide implants) could reduce the period of phototoxicity experienced by patients who have undergone photodynamic therapy with porfimer sodium.
Based on findings from 16 patients who received study treatment (9 MT-1, 7 placebo), patients treated with melanotan I experienced positive changes in their mood and mental health compared to placebo [8]. A secondary effect was reduced pain, which could have resulted in these changes.
A second follow-up trial was started in the same year and aimed to evaluate the safety of subcutaneous bioresorbable implants of CUV1647 (melanotan I). Results for this trial are not available [9].
Melanotan I has been investigated as a potential treatment for acne vulgaris. In 2011 a phase II randomized study was conducted in Germany to evaluate the efficacy and safety of two dosage regimens of subcutaneous bioresorbable afamelanotide implants in patients with mild to moderate acne vulgaris [10].
The study found that test subjects treated with melanotan I (either three injections at 3-week intervals, or two injections at 4-week intervals) experienced a decline in the number of inflammatory acne lesions on their faces. Researchers also found that quality of life as measured by DLQI improved in all patients from day 0 to day 56 and patients treated with melanotan I were able to spend up to seven times longer in direct sunlight without experiencing pain [10].
Another phase II randomized pilot study that aimed to evaluate the same melanotan I implant and narrow-band ultraviolet B (NB-UVB) light was also published in 2011. Results for this trial are not available [11].
Melanotan I has been investigated as a treatment for xeroderma pigmentosum (XP), an inherited condition characterized by extreme sensitivity to ultraviolet (UV) light. In 2019, a proof of concept, phase IIa open label study in Germany aimed to evaluate the safety and efficacy of melanotan I implants in patients with XP [12]. Another phase IIa study was started in 2021 and is currently ongoing [13].
A 2010 phase III, randomized, double blind, placebo controlled, parallel group study was undertaken in Germany, the Netherlands, and Belgium to evaluate the safety and efficacy of subcutaneous implants of melanotan I (16 mg) in patients suffering from polymorphic light eruption (PLE), a condition characterized by a rash following exposure to sunlight.
Researchers found that melanotan I could reduce the severity of PLE related pruritus when administered as 16 mg implants over a period of 4 months [14].
A 2011 phase III study in Europe aimed to confirm the safety and efficacy of subcutaneous bioresorbable melanotan I implants in patients with Erythropoietic Protoporphyria (EPP). The study aimed to determine whether 16 mg melanotan I implants could improve the quality of life of EPP patients. Researchers found that test subjects in the melanotan I group experienced less pain and a higher quality of life compared with those in the placebo group [15].
Based on findings from clinical studies, melanotan I appears to have a favorable safety profile. There have been no reported safety concerns, no significant drug-related adverse events, no deaths, and no adverse events leading to discontinuation of a study [8, 9, 10, 11, 12, 13, 14, 15].
Based on the research, the only side effects linked to melanotan I are:
Melanotan I is a research chemical and has no safe or recommended dosage. While data from clinical studies suggests that this peptide has a positive safety profile, there are several cases reported in the literature to show why experimentation with this peptide is limited to in vitro experimentation only [16].
Cousin et al. described a case of eruptive melanocytic naevi following melanotan I injection [17];
Evans-Brown et al. described the potentially harmful effects of melanotan I and melanotan II [18];
According to Langan et al. melanotan I use has been linked to changes in moles [19];
Dreyer et al. described a case of melanotan-induced priapism [20].
In summary, administration of melanotan I is restricted to clinicians and researchers.
For tanning of the skin, research suggests a melanotan I dosage range of 0.25mg to 2mg a day. It is advisable to start at the lowest possible dose, before increasing to achieve the desired outcome.
Researchers interested in studying the potential of melanotan I to treat a variety of skin disorders may consult the above-cited clinical trials to gain a fuller understanding of how this peptide has been dosed.
Melanotan 1 dosages ranging from 0.08mg/kg to 0.16mg/kg per day were implemented in phase I studies in Europe. The phase II and III European studies involved 16mg melanotan I implants for a treatment period of up to four months [8, 9, 10, 11, 12, 13, 14, 15].
Leading peptide researchers know the importance of proper supplies when safely handling Melanotan I.
To effectively include peptides in the research, a lab should be stocked with bacteriostatic water and alcohol prep pads, in addition to other essentials.
Generally, a researcher will need to acquire these supplies when conducting study on peptides like melanotan 1:
For researchers who do not have the required materials and supplies in the lab, checking with authorized sources to procure said products is required.
When administered as a sunless tanning agent, melanotan I is injected subcutaneously on a daily basis until the desired outcome is achieved.
Melanotan I powder should first be reconstituted using bacteriostatic or sterile water, before being injected subcutaneously into the fatty layer of tissue around the subject’s belly button area.
Melanotan I must be reconstituted with bacteriostatic or sterile water prior to being administered. It is important to follow all safety precautions during the reconstitution process, including wiping the tops of vials with alcohol wipes and avoiding contact with the syringe used to pull the bacteriostatic or sterile water.
For qualified researchers based in the United States, purchasing melanotan I as a research chemical is legal.
Melanotan I is a research peptide and should be administered with due care. While the peptide has exhibited minimal side effects in published research to date, researchers should note the general risks inherent to peptide administration.
Melanotan I has been shown to be an effective sunless tanning agent, as well as showing promise as a treatment for numerous skin conditions, across a range of studies to date.
No, melanotan I is not an anabolic androgenic steroid. It is a peptide analogue of alpha-melanocyte stimulating hormone.
No, melanotan I does not act to increase testosterone in test subjects.
No, melanotan I is not known to cause muscle gain in test subjects.
Apart from its well-known use as a sunless tanning agent, melanotan I is being actively investigated as a treatment of a variety of skin disorders. In clinical studies, it has been shown to reduce sunburn cells, pain in photodynamic therapy patients, and inflammatory acne lesions in patients with mild to moderate acne vulgaris.
Researchers interested in further exploring melanotan I will note that this peptide has a favorable safety profile and has not been linked to any serious adverse effects in test subjects.
If you are looking to order melanotan I for research purposes, head over to our preferred vendor here.
Disclaimer: Peptideinfo.net contains information about products that are intended for laboratory and research use only, unless otherwise explicitly stated. This information, including any referenced scientific or clinical research, is made available for educational purposes only. Peptideinfo.net makes every effort to ensure that any information it shares complies with national and international standards for clinical trial information and is committed to the timely disclosure of the design and results of all interventional clinical studies for innovative treatments publicly available or that may be made available. However, research is not considered conclusive. Peptideinfo.net makes no claims that any products referenced can cure, treat or prevent any conditions, including any conditions referenced on its website or in print materials.
To the extent that Peptideinfo.net references a product that is also a prescription medication, Peptideinfo.net does not does not offer medical diagnosis or treatment advice. The contents of Peptideinfo.net are intended exclusively for qualified researchers. Any individual seeking any advice on any prescription medication, or any disease or condition, is advised to refrain from using this site and consult their healthcare provider. Statements regarding products presented on Peptideinfo.net are the opinions of the individuals making them and are not necessarily the same as those of Peptideinfo.net.
Your access to Peptideinfo.net is subject to our terms of use.
© Peptideinfo.net. All rights reserved.